From the Departments of Dermatology and Pathology, Vanderbilt University, Nashville, Tennessee.
The author reports no conflict of interest.
Correspondence: Alan S. Boyd, MD, 719 Thompson Lane, Ste 26300, Nashville, TN 37204 (alan.boyd@vanderbilt.edu).
Favus is an uncommon form of tinea capitis (TC) currently seen in geographic areas with poor sanitation and limited access to health care such as emerging nations. Several variants of this condition have been described including one exhibiting a plaque composed of parchmentlike material. The makeup of this plaque has not been described. Tinea capitis is rare in adults, particularly when the infectious agent is Trichophyton rubrum, and affected patients often exhibit comorbidities associated with diminished immune surveillance. This case report describes an elderly woman with TC due to T rubrummimicking a rare form of favus.
Although favus is uncommonly seen in developed countries, it still exists and can mimick other conditions, notably cutaneous malignancies.
Favus may affect the skin and nails in addition to the hair.
The lesions of favus may persist for many years.
References
In 1909, Sabouraud1 published a report delineating the clinical subsets of a chronic fungal infection of the scalp known as favus. The rarest subset was termed favus papyroide and consisted of a thin, dry, gray, parchmentlike crust up to 5 cm in diameter. Hair shafts were described as piercing the crust, with the underlying skin exhibiting erythema, moisture, and erosions. Children were reported to be affected more often than adults.1 Subsequent descriptions of patients with similar presentations have not appeared in the medical literature. In this case, an elderly woman with tinea capitis (TC) due to Trichophyton rubrum exhibited features of favus papyroide.
Case Report
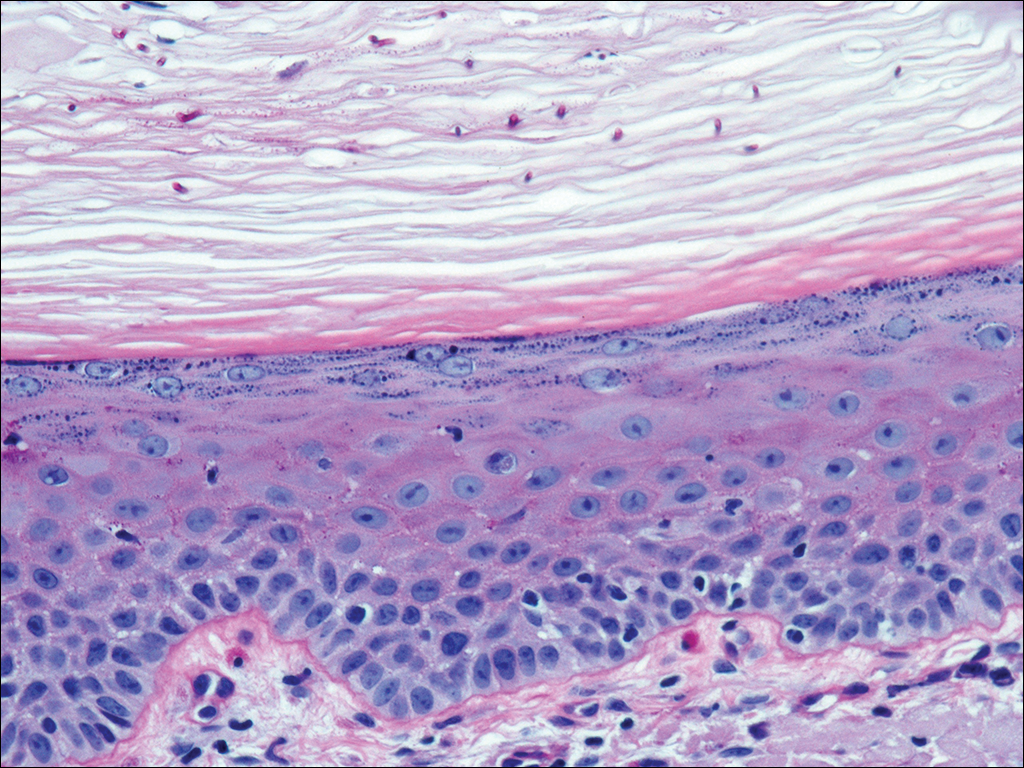
An 87-year-old woman with a long history of actinic keratoses and nonmelanoma skin cancers presented to our dermatology clinic with numerous growths on the head, neck, and arms. The patient resided in a nursing home and had a history of hypertension, osteoarthritis, and mild to moderate dementia. Physical examination revealed a frail elderly woman in a wheelchair. Numerous actinic keratoses were noted on the arms and face. Examination of the scalp revealed a large, white-gray, palm-sized plaque on the crown (Figure 1) with 2 yellow, quarter-sized, hyperkeratotic nodules on the left temple and left parietal scalp. The differential diagnosis for the nodules on the temple and scalp included squamous cell carcinoma and hyperkeratotic actinic keratosis, and both lesions were biopsied. Histologically, they demonstrated pronounced hyperkeratosis and parakeratosis with numerous infiltrating neutrophils. The stratum malpighii exhibited focal atypia consistent with an actinic keratosis with areas of spongiosis and pustular folliculitis but no evidence of an invasive cutaneous malignancy. Periodic acid–Schiff stains were performed on both specimens and revealed numerous fungal hyphae within the stratum corneum (Figure 2) as well as evidence of a fungal folliculitis.
Figure 1. A white-gray plaque of tinea capitis on the crown with erythema and alopecia at the back edge of the plaque.
Figure 2. One of the initial biopsies from the left temple demonstrated mild keratinocyte atypia and numerous fungal hyphae within the stratum corneum (periodic acid–Schiff, original magnification ×400).
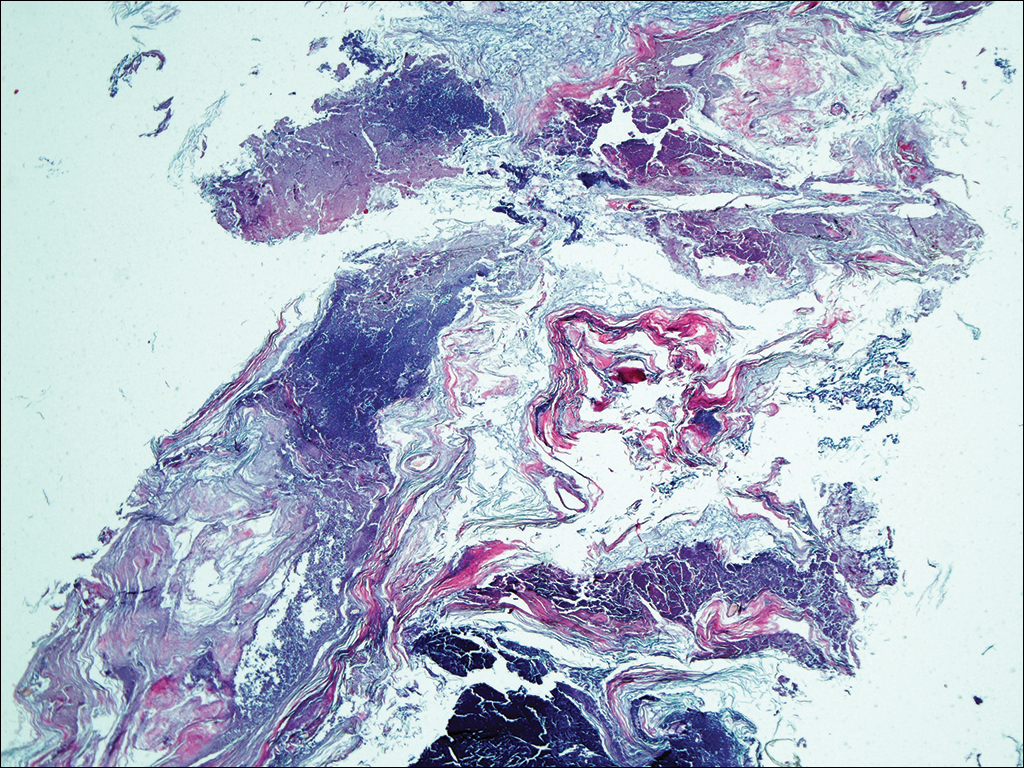
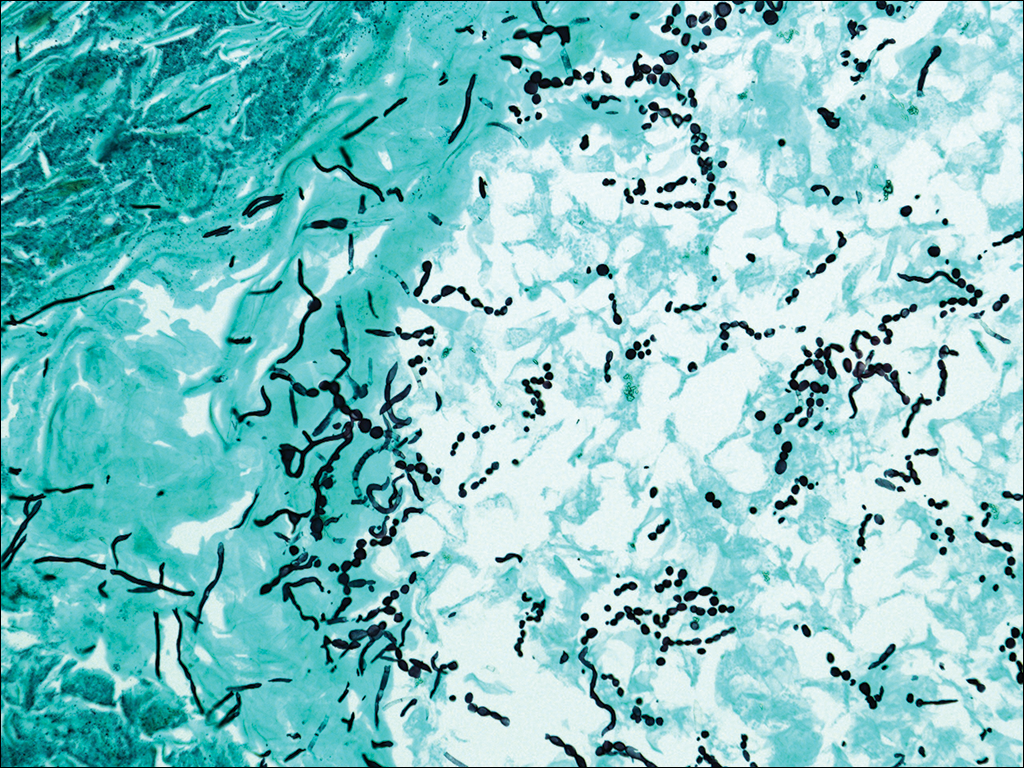
At a follow-up visit 2 weeks later, a portion of the hyperkeratotic material on the crown of the scalp was lifted free from the skin surface, removed with scissors, and submitted for histologic analysis and culture. The underlying skin exhibited substantial erythema and diffuse alopecia. The specimen consisted entirely of masses of hyperkeratotic and parakeratotic stratum corneum with numerous infiltrating neutrophils, cellular debris, and focal secondary bacterial colonization (Figure 3). Fungal hyphae and spores were readily demonstrated on Gomori methenamine-silver stain (Figure 4). A fungal culture from this material failed to demonstrate growth at 28 days. The organism was molecularly identified as T rubrum using the Sanger sequencing assay. The patient was treated with fluconazole 150 mg oncedaily for 3 weeks with eventual resolution of the plaque. The patient died approximately 3 months later (unrelated to her scalp infection).
Figure 3. Low-power view of the parchmentlike plaque atop the scalp exhibited occasional hair shaft fragments with massive hyperkeratosis and infiltrating inflammatory cells (H&E, original magnification ×4).
Figure 4. Gomori methenamine-silver stain of the scalp plaque demonstrated numerous fungal hyphae and spores (original magnification ×200).